Pain is a universal human experience and the most common reason people
seek medical care. In many cases pain tells us something is wrong, that tissue in our
body has been damaged, and we need to do something to change the
situation.
PAIN - Some definitions you should know: Algesia: Is your sensitivity to pain.
Analgesia: Absence of pain in response to stimulation which would normally be painful.
Hypoalgesia: Diminished pain in response to a normally painful stimulus.
Hyperalgesia: Increased response to a stimulus which is normally painful.
Allodynia: Pain due to a stimulus which does not normally provoke pain.
Pain Threshold: The least experience of pain which a subject can recognize.
Pain Tolerance Level: The greatest level of pain which a subject is prepared to tolerate.
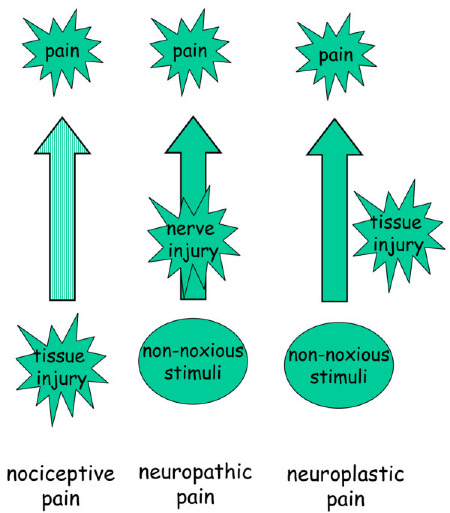
There are 3 possible scenarios when pain or tissue damage is present:
2. Analgesia - Tissue damage occurs without causing pain NO OR REDUCED FEELING OF PAIN - this scenario will not be discussed much. Destructive (can be due to nerve damage - Neuropathy- very dangerous)
3. Non-Nociceptive - Pain occurs in the absence of new tissue damage or with very little tissue damage. Destructive changes in the nervous system. (Chronic Pain) Two main types 1. Neuropathic and 2. Neuroplastic pain
1. Nociceptive Pain AKA Warning Pain (Tissue damage and pain) Nociceptive pain results from tissue damage.
Warning pain is the
expected pain associated with an underlying disease process or tissue damage.
Tissue Damage:
1. Chemical 2. Thermal 3. Mechanical
The source of the warning pain is usually easily determined. Such as a chemical irritation, burn, cut, bruise, abrasion, laceration, pulled muscle, organ pathology or other tissue damage. This is a warning sign that tissue damage is occurring.
As stated earlier the term "acute pain" has been
replaced by the term "warning pain". Warning pain is the expected pain associated
with an underlying disease process or tissue damage. In the past "acute pain" has been arbitrarily
dictated as lasting anywhere from a few days to 3 months. This arbitrary time
frame for when acute pain becomes chronic pain has little scientific basis. The term warning pain on the other hand describes the physiological purpose of the pain.
Warning pain is generally helpful for us because it is a sign of tissue
damage or danger. Over millions of years, the nervous
system has developed the ability to experience pain as a protective system to
warn us of imminent dangers and to keep us out of trouble. The severity of the
pain is not related to tissue damage. In other words, one person may have
significant tissue damage with little pain, while another person may have very
little tissue damage with significant pain.
2. Analgesia (Tissue damage and NO pain)
Absence of pain in response to stimulation which would
normally be painful. Usually due to nerve damage, paralysis, spinal cord injury or progressive neuropathy.
Peripheral neuropathy is caused by damage to your body’s peripheral
nerves. This damage disrupts the body’s ability to communicate with its
receptors, muscles, skin, joints, or internal organs. It is like the
body’s
wiring system breaking down.
3. Non-nociceptive pain (NO local tissue damage but pain is present) Pain comes from within the nervous system. A. Neuropathic B. Neuroplastic
A. Neuropathic Pain Examples: RSD, MS, CRPS, Carpal Tunnel Syndrome, Neuroma, Tumor, or Herniated Disc
Neuropathic
pain results from damage to or dysfunction of the peripheral or
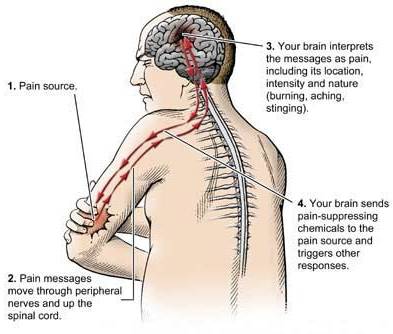
central nervous system, rather than stimulation of pain receptors. With neuropathic pain, the nerve fibers
themselves may be damaged, dysfunctional or injured. Originating from either the peripheral nervous system (the nerves in
the area between the tissue and the spinal cord) or the central nervous
system (the nerve connecting the spinal cord to the brain).
Neuropathic
pain can be caused by a multitude of reasons, such as nerve
inflammation, nerve degeneration (examples include stokes and multiple
sclerosis), nerve pressure, and nerve infection. If ignored, neuropathy can lead to
numbness, pain, weakness and incoordination. There are more than 100
known types of peripheral neuropathy, each with
its own characteristic symptoms, pattern of development, and prognosis. Approximately 30% of neuropathy cases are linked to diabetes. Other
common causes of neuropathy include autoimmune disorders, tumors,
hereditary conditions, nutritional imbalances, infections or toxins.
Another 30% of neuropathies are termed “idiopathic” when the cause is
unknown.These damaged nerve fibers
send incorrect signals to other pain centers.
B. Neuroplastic Pain Changes occur within the nervous system that result in pain with little or no tissue damage. This type of pain is neurologically progressive and can become independent of the original pathology that caused pain.
Your pain warning system is not just a system for the
conduction of pain impulses from the periphery to the brain. Scientists now
know that changes can take place in the receptors,
nerves, the spinal cord and in the higher brain centers following injury,
inflammation, continued use of the pain system, disuse of inhibiting factors
and learned behaviors. These changes can increase the likelihood that pain is
perceived and may contribute to the development of "chronic pain". Therefore,
"chronic pain" can in some cases be considered a separate disease, independent of
the pathology that initially set off the pain warning system.
The nociceptive (pain) system is not just a system for the conduction
of pain impulses from the periphery to the brain. We now know that
plastic changes can take place in the periphery, the spinal cord and
also in higher brain centers following injury or inflammation. These
changes may increase the magnitude of the perceived pain and may
contribute to the development of chronic pain syndromes. SWISS MED WKLY
2002;132:273– 278
There is good
evidence that chronic pain is associated with changes in brain function. It is
possible that these brain changes compound chronic pain and future agents may
be able to prevent such complications. German J Psychiatry 2003; 6: 8-15